|
Keywords:
|
Sudden death,Ventricular
fibrillation,Ventricular tachycardia,Cardiac arrest,Exercise tests
|
|
Author
Block:
|
Theodore
Chow, Edward J Schloss, Theodore J Waller, Eugene S Chung, Santosh G Menon,
Terri Booth, Alena Goldman, Erin Ely, The Lindner Center/Ohio Heart Health
Center, Cincinnati, OH; Richard Cohen, Massachusetts Institute of Technology,
Cambridge, MA; Dean J Kereiakes; The Lindner Center/Ohio Heart Health Center,
Cincinnati, OH
|
|
Background: The Multicenter Automatic
Defibrillator Implantation Trial II (MADIT II) showed survival benefit from
defibrillator (ICD) implantation in patients with coronary disease and EF <30%.
We prospectively evaluated whether T-wave alternans (TWA), a non-invasive
marker of ventricular tachyarrhythmic risk, could identify lower risk MADIT
II type patients.
Methods: Patients (n=203) with coronary disease and EF <30%
underwent TWA testing primarily by treadmill exercise. A positive TWA was
defined as sustained alternans >1.9μV with an onset heart rate <110 bpm
in 1 orthogonal or 2 contiguous chest leads. Patient management was according
to physician discretion. Follow-up was achieved for 193 patients. A
ventricular tachyarrhythmic event (VTE) was defined as an arrhythmic death,
resuscitated cardiac arrest or appropriate ICD discharge. Endpoint events
were analyzed blindly with respect to TWA outcomes. Data was processed using
Kaplan-Meier analysis in conjunction with a single-sided log rank test of
significance.
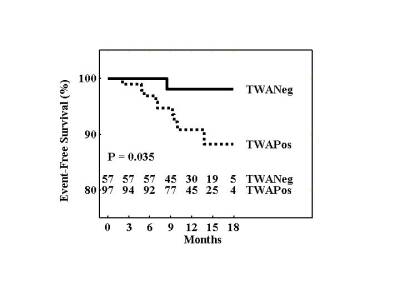
Results: Results of TWA testing were: positive in 97 (50.3%), negative
in 57 (29.5%), and indeterminate in 39 (20.2%). During a mean follow-up of
375 ± 119 days there were 16 deaths (9 arrhythmic), 4 appropriate ICD
discharges and no resuscitated cardiac arrests. VTEs occurred in 9 TWA
positive patients, 1 TWA negative patient, and 3 TWA indeterminate patients.
The event rate to 18 months was 11.8% (SE 3.9%) and 2.0% (SE 1.9%) among TWA
positive and negative patients respectively; Relative Risk = 6.0 (p=0.035).
Conclusions: TWA identifies MADIT II type patients at lower risk of
VTEs and may guide more cost effective deployment of ICD resources.
|
