|
Daniel J. Cantillon, MD,
Daniel P. Morin, MD, Eran S. Zacks, MD, Kenneth M. Stein, MD, Steven M.
Markowitz, MD, Suneet Mittal, MD, Bindi K. Shah, MD, Matthew Janik, MD, Shaun
Ageno, MD, Andreas C. Mauer, MD, Bruce B. Lerman, MD and Sei Iwai, MD.
Cornell University Medical Center, New York, NY
|
|
Background: Microvolt
T-wave alternans (TWA) has been proposed as a risk-stratifier in ischemic
and non-ischemic cardiomyopathy (CM) pts. We prospectively evaluated the
utility of TWA testing in predicting arrhythmia-free survival in this
population.
Methods: We enrolled 268 consecutive pts (66 ± 11 yrs; 217 M [81%])
with ischemic or non-ischemic CM and EF ≤ 35% who underwent
electrophysiologic testing and TWA testing and who were followed for
≥ 12 mos. TWA was performed by atrial pacing @ 550 ms or by treadmill
testing, and interpreted using standard criteria. Positive and
indeterminate results were grouped as non-negative. Pts were followed by
telephone interview, hospital admission, clinic follow-up, and Social
Security Death Index. The primary endpoint was arrhythmia-free (VT/VF) survival.
Secondary endpoint was total mortality.
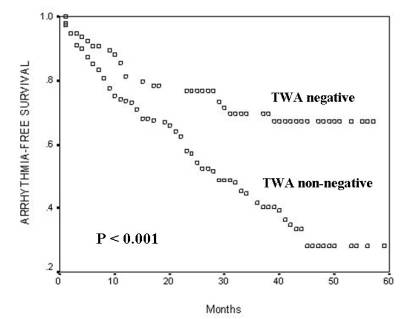
Results: 208 (78%) pts had ischemic CM and 60 (22%) had non-ischemic
CM. The mean EF was 26 ± 7%. Pts were followed for 33 ± 14 months. TWA was
negative in 78 pts (29%), and non-negative in 190 pts (71%). Life-table
analysis demonstrated substantially better arrhythmia-free survival in TWA
negative pts when compared with non-negative (p<0.001; see figure).
There was no difference in ICD implant rates between TWA-negative and
non-negative pts (65% vs 71%; p=0.84). Despite substantial ICD implant
rates in this population, total mortality was high, albeit lower in the
TWA-negative group (overall p = 0.05; 2 yr rate = 17 vs 28%). TWA had a
negative predictive value (PV) of 77% for 2-yr arrhythmia-free survival and
positive PV of 43% for 2-yr mortality.
Conclusions: Microvolt TWA testing is effective in predicting
arrhythmia-free survival and all-cause mortality in a SCD-HeFT population.
Although a negative TWA predicts event-free survival, the event rate in
this group is sufficiently high to still warrant consideration of an ICD.
|
|
|
